
When treating patients with T2DM, one of the main challenges physicians face is understanding the complexity of individual patient profiles. This complexity arises not only from the multidimensional nature of T2DM itself, but also from the multitude of associated comorbidities and underlying pathophysiological processes14,15. It implies that course of the disease can be highly variable. While some patients with T2DM face rapid deterioration, others maintain stable for extended period of time. This makes long-term planning challenging16.
Recognizing the important role of inflammation in the T2DM pathophysiology and its associated comorbidities has highlighted the need to identify groups of patients prone to increased inflammation as well as to identify risk factors associated with increased inflammatory responses17. In this way clinicians can more effectively adjust therapeutic approaches and provide better control of the disease that extends beyond glucose control.
According to the authors’ best knowledge, the studies that applied clustering method to group the patients with T2DM targeting inflammation, comorbidities and therapy regimens are scarce. We found only one study that used clustering to pair inflammatory and clinical parameters in patients with T2DM. However, it was conducted on a considerably smaller sample size than our study14.
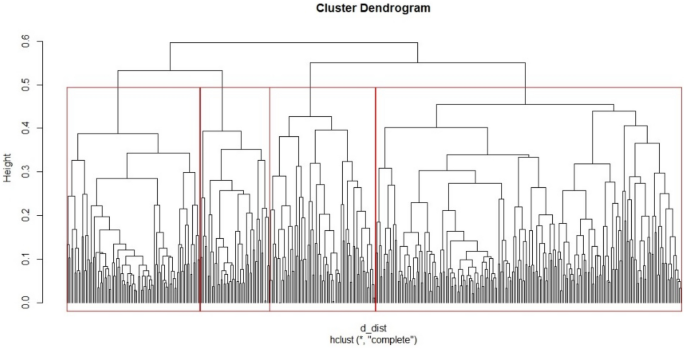
We identified four distinct profiles of patients with T2DM based on their clinical and demographic characteristics. Each cluster had its unique characteristics and differed in terms of age, disease duration, associated conditions, and biochemical profiles. The Cluster 3 featured the oldest patients with the longest duration of T2DM, who also had the lowest levels of GFR and exhibited poor glycemic control. Patients from this cluster had the highest level of NLR and PLR which means that the Cluster 3 had the most pronounced subclinical inflammation since the correlation between increased NLR and PLR values and inflammation in T2DM is well established in the literature18. These findings are in alignment with other studies suggesting that inflammation might be associated with a more advanced or prolonged stage of T2DM, poor glycemic control and low GFR19,20,21,22.
T2DM is considered to be age-related disease. It is characterized by chronic activation of the innate immune system which can be increased by over-nutrition and aging process23. Over-nutrition in addition to genetic predisposition and lack of physical activity leads to obesity. Particularly in cases of central adiposity, this can trigger adipose tissue dysfunction, prompting macrophage infiltration and a subsequent surge in inflammatory cytokine release24. Chronically elevated inflammatory biomarkers promote insulin resistance and hyperglycemia. Furthermore, chronic hyperglycemia sustains persistent inflammation creating a cycle where inflammation exacerbates glucose metabolic disturbances, further aggravating the body’s metabolic equilibrium24. This can explain why patients with higher levels of HbA1c like in the Cluster 3 exhibit the higher level of inflammation, as determined by higher NLR, PLR and neutrophil count.
Chronic hyperglycemia and inflammation have detrimental effects on various organs including kidneys25. These effects manifest as changes in the microvasculature, particularly in the thickening of the capillary basement membrane impacting arterioles in the glomeruli, retina, myocardium, skin, and muscle. Such alterations in the glomeruli play a crucial role in the onset and progression of diabetic nephropathy6. In a recent study, it was found that an increased NLR and PLR were not only significantly correlated with diabetic nephropathy but were also proposed as predictors and prognostic risk markers of diabetic nephropathy26. Our findings align with this, highlighting the interrelationship between kidney function and inflammatory responses. Specifically, once kidneys are damaged, they can further exacerbate inflammatory responses in the body27. This interplay is reflected in the Cluster 4, where good kidney function corresponds well with moderate inflammation markers, potentially suggesting a protective mechanism against intense inflammation. Furthermore, the Cluster 3 had the highest percentage of patients diagnosed with diabetic nephropathy and coronary disease. Previous studies also showed that higher NLR level was associated with an increased prevalence of CVD and diabetic nephropathy pointing out the important role that inflammation plays in development of such complications28. The coexistence within a single cluster highlights their interconnected nature6,7.
Patients in Cluster 4, who are characterized with the best clinical performances, have higher mean level of inflammation (as indicated by NLR and PLT markers) than patients in Cluster 1 (who have lower renal function and more CVD and worse metabolic indicators) but this difference did not reach statistical significance. Another feature of the clusters is the fact that patients in Cluster 4 have significantly lower level of inflammation (as indicated by NLR and PLT markers) than patients in Cluster 3, who are the worst with respect to the presence of CV comorbidities, and are also the oldest ones. One of the possible reasons for such discrepancies includes the wide range of age of studied diabetic patients that could have influenced the characteristics of clusters, in addition to differences in medications use. Furthermore, there are complex relationships between age, gender, postmenopausal status, T2DM duration, body shape, BMI categories, HbA1c, and inflammatory marker values as observed in previous studies29,30.
Although the Cluster 3 had the highest levels of inflammatory markers, we observed paradoxically low levels of total cholesterol and LDL. Considering the high prevalence of coronary artery disease in the Cluster 3, it might be plausible that these patients have been treated aggressively with lipid-lowering therapies in the past or might still be under such treatment.
Notably, the Cluster 3 also demonstrated a pronounced percentage of retinopathy cases, although this association did not reach statistical significance. These results are in line with a study conducted by Ciray et al.31 that found no independent association between NLR and diabetic retinopathy. While some research has suggested NLR as a potential diagnostic biomarker for diabetic retinopathy, the association remains debated28. The highest percentage of patients with diabetic neuropathy was in the Cluster 2 which also had the pronounced levels of NLR and PLR but significantly lower than in the Cluster 3. This could be explained by multifactorial nature of the retinopathy and neuropathy where inflammation is just one aspect of a broader pathophysiological picture32.
Furthermore, it’s worth noting that Cluster 4 which included the youngest patients with the lowest levels of fasting glycaemia and HbA1c, along with the highest GFR and relatively short disease duration presented with surprisingly higher inflammation markers compared to Cluster 1. Patients from the Cluster 1 also showed some unfavorable characteristics like patients from Cluster 2 and 3 including older patients with high percentage of hypertension and decreased GFR who had the worst glycemic and lipid control. Yet, despite these seemingly adverse factors, this cluster surprisingly exhibited the lowest levels of inflammatory markers. Medication regimen could be a contributing factor to these observed levels of inflammation in the Cluster 1. Namely, these group of patients had the highest percentage of patients on oral therapy, with Metformin being the most commonly used. Even though there was not a statistically significant difference between the clusters regarding Metformin use, we believe its presence played a pivotal role in reducing inflammation levels as suggested in different studies which showed that Metformin has potent anti-inflammatory effect through inhibiting secretion of pro-inflammatory cytokines from activated macrophages33,34. In accordance with this, study by Mohammed et al.35 revealed a dose-dependent effect of Metformin on the reduction of NLR in T2DM patients. Furthermore, Cluster 1 had the highest percentage of patients using sulfonylureas, which also appear to have some anti-inflammatory effect but less potent than metformin36. Despite the documented anti-inflammatory properties of insulin evidenced by both in vitro and animal studies—such as modulation of molecular pathways, reduction of pro-inflammatory cytokine expression, and augmentation of anti-inflammatory mediators—this cluster had the lowest percentage of patients using insulin37.
The Cluster 1 had the highest percentage of patients using Angiotensin-Converting Enzyme Inhibitors. These drugs, while primarily recognized for their antihypertensive effects, also exhibit anti-inflammatory, antiproliferative, and antioxidant properties through their action on angiotensin II receptors38. This could have further contributed to the reduced inflammation levels observed in this cluster. Although with the lowest levels of inflammatory markers, patients from the Cluster 1 still had the higher percent of patients with diabetic complications, especially coronary artery disease compared to Cluster 4. It is possible that current snapshot of inflammatory markers might not provide a comprehensive history and inflammation may have decreased over time, perhaps due to medication or lifestyle modifications still resulting in coronary artery disease from previously elevated inflammation. However, it is crucial to emphasize that the Cluster 3 showed the highest level of inflammation and had the most pronounced incidence of coronary artery disease. This correlates with findings from prior research indicating that an elevated NLR is closely associated with the progression of coronary atherosclerosis. Increased ratios typically align with a deteriorating cardiovascular risk profile and increased complexity and severity of coronary artery disease confirming the established relationship between inflammation and cardiovascular complications in T2DM patients39.
We expected a higher percentage of patients to be using medications with proven cardiovascular and renal benefits (SGLT2i, GLP-1r) in Cluster 3, as it had the highest percentage of patients with renal impairment and coronary heart disease40. These drug classes have shown superiority in terms of cardiovascular and renal outcomes compared to DPP4i in patients with T2DM, as demonstrated in a meta-analysis that included 23 cardiovascular outcome trials41. However, in addition to Metformin, patients from this cluster more commonly used DPP4i. Other studies have yielded similar results, indicating that despite the proven benefits of SGLT2i and GLP-1r, physicians predominantly continue to prescribe DPP4i. This trend can be explained by clinical inertia42.
Our study had some limitations. The first limitation is a cross-sectional design of the study since it allows us to observe association between variables, but it limits us when making casual conclusions. Also, the wide range of age of diabetic patients included in the study could have influenced the characteristics of clusters. Another limitation derived from record based data, because there might be inaccuracies or missing information from medical records. For instance, there could be potential underreporting or misclassification of some clinical conditions based on the ICD-10 codes. While use of prescribed medication was recorded we did not provide data about dietary habits and consumption of over the counter drugs which could both influence inflammation levels.
In conclusion, it is worth to note that inflammation is one of the key contributors to disease T2DM pathophysiology and it is associated with variables like age, disease duration, glycemic control, kidney function and medication regimens. Still, it is important to emphasize that inflammation is not the only factor contributing to the development and progression of T2DM and its complications. Other factors like genetic predisposition, comorbidities, lifestyle choices, changes in metabolic control over the time all play significant role in disease progression. This also emphasizes the need to personalize approach in managing T2DM. In that sense, the identification of these distinct clusters provides invaluable insights. Beyond glycemic control, an integrated approach considering inflammation, vascular health, renal function, and other comorbidities is crucial. Further studies are needed to validate and expand these observations.

 Arabic
Arabic Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish