
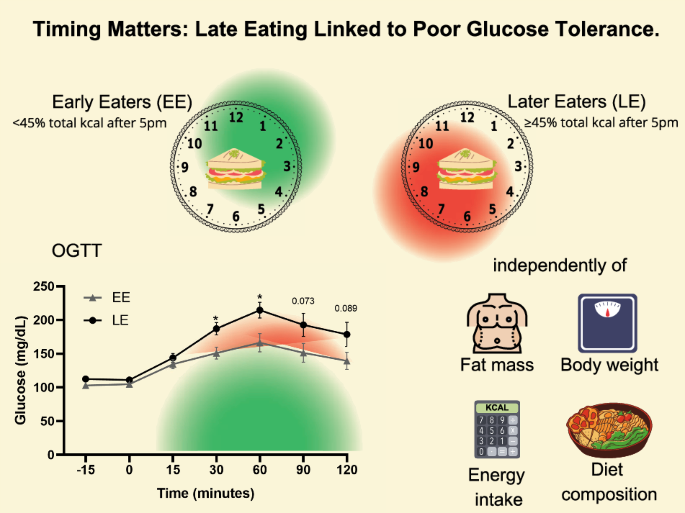
The main finding of this study is that increased energy intake after 5:00 pm is independent of increased body weight or fat mass, diet composition, or increased energy intake, and that increased energy intake after 5:00 pm is associated with obesity and managed with diet or metformin. It is associated with decreased glucose tolerance in adults with prediabetes or T2D.
Our data support the association between late eating and impaired glucose tolerance shown in previous studies in non-obese individuals [1]. Adds to previous research on negative effects of late eating on BMI and metabolism [2] And its connection to poor eating habits [2, 3]we now observed that the association between LE and impaired glucose tolerance was independent of reduced body weight, fat content, caloric content, or diet composition.
Previous studies have linked eating later in the day to lower glucose metabolism, with people who eat later in the day having higher BMI and higher body fat. [5, 6]not only does the feeling of fullness decrease and the feeling of hunger increases; [7, 8] This may explain their high daily calorie intake. Compared to the morning, foods consumed in the evening are generally more energy-dense, resulting in a higher overall total energy intake. [2]this may explain why late eating is associated with increased body weight and fat mass. Therefore, the glucose benefits observed when distributing energy intake earlier in the day may be explained by reduced body weight. However, even among people who report the same total daily caloric intake, slow eaters may have a higher BMI/fat mass, lower glucose metabolism, and lower caloric intake. regardless, it highlights the potential role that meal timing itself has on metabolic decline. [9,10,11,12].
Our study shows that older adults with prediabetes or early T2D and slow eating habits have poor glucose tolerance, independent of body weight, fat content, and energy intake. This is consistent with short-term intervention studies (1-14 days) in healthy volunteers. Participants who consumed an isocaloric diet aimed at stabilizing their weight showed decreased glucose tolerance and decreased resting energy expenditure when calories were consumed later in the day. [13, 14]. This may be related to the previously reported higher postprandial glycemic response after dinner compared to breakfast. [14,15,16]. The importance of late eating on glucose was also shown in a prospective observational epidemiology study of 2,642 women at risk for T2D, which found that eating after 9pm increased the risk of developing T2D over 5 years. It is said to be 1.5 times more expensive. [17].
Interventions that combined caloric restriction with a morning versus afternoon distribution of glucose and HbA1C in daily caloric intake resulted in greater reductions, and insulin responses were higher in the morning than in the evening on caloric intake days. [18, 19]highlighting the importance of meal timing in glucose metabolism in T2D patients. However, another weight loss study of 23 people with obesity and prediabetes or T2D found no difference in weight or metabolism when 50% of total daily calories were consumed in the morning and evening. . [20].
Diet composition is also a well-established determinant of T2D risk. Observational studies have shown that slow eaters tend to choose highly processed, high-carbohydrate and high-fat meals in the evening. [2, 3]. Our research supports those findings. LE consumed more carbohydrates and fat after 5pm compared to EE. This behavior has previously been associated with worsened nocturnal glucose metabolism and may cause desynchronization of the peripheral circadian system. [2] It can cause glucose intolerance to worsen further.
Biases and limitations include inclusion criteria for the NY-TREAT study [4]The focus on individuals with a feeding window of 14 hours or longer introduces potential bias. However, the data may still be representative given the prevalence of such dietary patterns in the general population. Despite real-time data collection via a smartphone app, there remains an element of self-reporting as participants must remember to take photos of their meals, but validation shows an error rate of at least 10%. It is suggested that there is [3]. Although the small sample size of this study is a limitation, prior power calculations are not always possible in pilot studies such as this. However, this cohort specifically targeted individuals with prediabetes or T2D and obesity, so caution should be taken when generalizing the results. Replicating the study with more diverse populations and age groups would increase external validity and contribute to a broader understanding of the applicability of the results beyond the demographics studied.

 Arabic
Arabic Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish