
Table of Contents
Study design
We performed a study to assess the feasibility of a teleintervention on mental health parameters of patients with type 1 diabetes during an outbreak. Previous databases were used to identify potential participants for the study, which refer to databases of main institutions where patients with type 1 diabetes undergo outpatient follow-up and contained information on telephone number and recent glycated hemoglobin (HbA1c) assessment. A medical record review was later performed to identify those who met the inclusion criteria for the study. Potential participants were contacted by telephone and invited to participate in the study, and an inclusion in the protocol was performed at that time to respect social distancing measures.
Participants
Individuals with a previous diagnosis of type 1 diabetes with regular follow-up in two public care centers in Southern Brazil were selected. Patients aged ≥ 18 years and with a measurement of HbA1c between January and March 2020 were included. The exclusion criteria were patients who had a medical history of any condition that prevented their understanding of the questionnaires (such as dementia) and interaction with researchers by telephone (such as deafness). Institutionalized and hospitalized patients at the time of inclusion were also not included. Previous diagnoses of mental health disorders were not considered inclusion or exclusion criteria.
Enrollment and study procedures
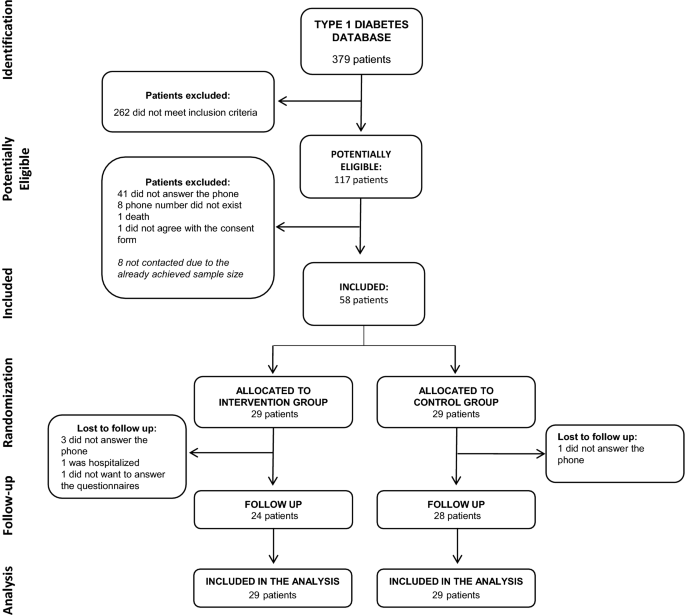
Enrollment began on April 14, 2020 and ended on April 29, 2020. The first confirmed case of COVID-19 in Brazil was on February 26, 2020, and the formal recommendation for social distancing for risk groups in Southern Brazil (Porto Alegre city) started on March 22, 2020. Thus, patients were included in the study approximately 2 months after the first case of COVID-19 in the country and 1 month after the beginning of the contact restriction measures. For the identification of potential participants for enrollment, a list of all patients with type 1 diabetes mellitus who underwent follow-up at the study institutions between January 2016 and December 2019 was assessed. These participants initially identified had their electronic medical records reviewed, and those who met the inclusion criteria and had an updated telephone number were randomly contacted via telephone to invite them to participate in the study. The enrollment procedure stopped when the number predicted in the sample size calculation was officially included in the study. The details of this procedure are fully described in Fig. 1.
Flow diagram of the study.
An inclusion questionnaire was applied when the participant was enrolled into the study. Randomization was performed for patients with type 1 diabetes in enrollment into the study, in a 1:1 ratio that was provided by the Randomization.com website. The electronic system generated randomization patterns for the sequence of inclusion of participants with type 1 diabetes in the study. The main researcher was responsible for generating the randomization patterns, which were performed before inclusion of participants in the study. Participants were randomly contacted, without any prior knowledge of them by the research team, and then allocated to each group based on their inclusion number and the pre-established allocation pattern. Participants who were enrolled received a second call to start the intervention procedures or to receive guidance on an educational website that was available to the control group.
Teleintervention characteristics
A multidisciplinary team composed of 6 members (2 general practitioners, 1 endocrinologist, 1 nutritionist, 1 physical educator, and 1 psychologist) was responsible for preparing protocols for appointments that were performed remotely. The original clinical trial design envisaged a similar intervention for patients with type 1 diabetes or type 2 diabetes12. However, all protocols were customized for the particularities of type 1 diabetes. The objective of this strategy was to provide guidance tools and to represent a support channel for the needs of patients with type 1 diabetes during the COVID-19 outbreak. The interface protocols used are available as supplementary material.
For the maintenance of remote connections, a group of moderators, which corresponded to postgraduate students and graduate students, was responsible for mediating contact between the patients and the multidisciplinary team, as pre-planned in the initial protocol. In this study, the intervention was moderated by experienced professionals, who were attending a postgraduate course (JA, DWF, GHT, TRC). The moderators went through a training process to qualify them to make the proposed remote appointments. Then, these moderators were responsible for performing the weekly teleinterventions and discussing potential questions regarding the participants with the multidisciplinary team. An online instant messaging group was created so that the multidisciplinary team could instantly respond to the moderators’ demands. The moderators were responsible for transmitting the information to participants, and there was no direct contact between the multidisciplinary team and the patients included. The participants were assigned to a specific moderator, who accompanied the same participant throughout the intervention. The assignment was performed based on the participant inclusion number, matching with a list of moderators in alphabetical order.
The duration of the proposed intervention was 16 weeks. The main pillar of this intervention was the provision of weekly telephone contacts between patients and health professionals. Each remote appointment was scheduled to last about 10 min and aimed to address different topics related to the control of diabetes, the presence of emotional overload, and the maintenance of healthy habits during the outbreak.
In addition to developing the protocols, the multidisciplinary team was also responsible for addressing diabetes care demands during the study period. Moderators could access the multidisciplinary team at any time during the follow-up period to address specific patient demands. During the remote contacts, patients were routinely asked for reports on glycemic controls, and were encouraged to maintain good adherence to treatment during each call. Prescription adjustments were discussed with an endocrinologist if recurrent hypoglycemia was reported.
Participants who were randomized to the control group received the usual care during the outbreak, in accordance with the pandemic-related restrictions. For this group, a website was made available with recommendations about maintaining healthy habits during crisis situations. This proposal aimed to offer a reliable source of information during the outbreak for these participants without interacting directly with them.
Outcome measures
Emotional disorder outcomes and changes that occurred during the pandemic were assessed using specific questionnaires, which were applied via telephone calls. All participants were evaluated when they were enrolled into the study (baseline) and after 16 weeks of intervention (follow-up). For the evaluation of the study outcomes, telephone calls were made for the application of the questionnaires by the group of researchers of the project, and moderators were not responsible for applying the questionnaires to their respective patients. Subsequently, a physician blinded to the participants responses was responsible for evaluating the questionnaire final scores.
The study outcome was the assessment of recruitment capability and adherence to the proposed intervention (feasibility outcome). Moreover, we evaluated the presence of a positive screening for emotional disorders at the 16-week follow-up. The Brazilian version of the Self Report Questionnaire-20 (SRQ-20) was used for this evaluation, and a positive screening result was considered if the score was ≥ 713. The choice of this questionnaire was based especially on the wide range of psychiatric disorders that it assesses (anxiety disorders, depression, and somatoform disorders) compared to other mental health scores. In addition, an assessment of differences between the groups for diabetes-related emotional distress, eating disorders, and sleep disorders was performed using screening tools. The Brazilian version of the Problem Areas in Diabetes Scale (B-PAID) was used to evaluate diabetes-related emotional distress (considered positive if the score was ≥ 40)14. The Brazilian version of the Eating Attitudes Test (EAT-26) was used to assess eating disorders (considered positive if the score was ≥ 20)15. The Brazilian version of the Mini Sleep Questionnaire (MSQ) was used to evaluate sleep disorders screening (considered positive if the score was ≥ 31)16.
Finally, an evaluation of patients’ perceptions (subjective assessment of changes that occurred with the pandemic in relation to eating habits, physical activity, glycemic control and mental health) was performed as pre-planned in the protocol. For this assessment, participants were asked to give a score (0 to 10) for adherence to diet, maintenance of physical activity, glycemic control, and mental health according to their impression before and during the pandemic (follow-up period). Moreover, psychosocial aspects and perceptions about diabetes care during the pandemic were assessed by asking the participants about the presence of respiratory symptoms. Finally, social distancing measures, financial and medical assistance difficulties that may have occurred during the outbreak period were asked with yes/no answer options.
Demographics and clinical data
Personal information, such as age, marital status, race/ethnicity, diabetes duration, disease complications, current medications, and psychiatric history were obtained from each patient’s medical records and then verified by the participant. The HbA1c (high-performance liquid chromatography method) result was obtained from records and collected between January and March 2020. Diabetes complications were evaluated using the presence of retinopathy, which was considered based on the last fundus examination. For neuropathy, the presence of a previous diagnosis or an altered monofilament 10-g test result at a medical appointment was considered. For diabetic kidney disease, the presence of macro/microalbuminuria or glomerular filtration rate lower than 60 ml/h registered in medical records were considered. A history of coronary heart disease, stroke, heart failure, or peripheral arterial disease that was recorded in the patients’ medical records indicated cardiovascular disease.
Power estimations
This study was designed to assess the feasibility of the proposed teleintervention, which was designed to improve mental health parameters in patients with type 1 diabetes. We performed the sample size calculation for two-sample design according to the superiority by a margin test for difference between two proportions described by Chow et al.18. A previous study found that, with the use of a remote intervention in patients with type 1 diabetes, changes were significantly greater in the intervention group compared to a control group. Assuming that 28% of the subjects in the control group and 64% in the intervention group improved mental health parameters with a remote teleintervention17, and after applying continuity correction, the study would require a sample size of 45 individuals for each group to achieve a power of 80% and a level of significance of 5% for declaring that the intervention is superior to the control group at a 10% margin of superiority.
Statistical analysis
We used SPSS v.22 software (IBM Corp., Armonk, NY, USA) software for the analyses. Participants’ characteristics data were reported as the mean ± standard deviation (SD) if the data were normally distributed. Differences between groups for baseline data were evaluated using an unpaired t test and the Mann–Whitney U test for continuous variables and the Chi-square test was used for categorical variables.
Data related to adherence and feasibility of the proposed intervention are presented descriptively. Furthermore, secondary data were analyzed using the intention‐to‐treat principle. We used the Markov Chain Monte Carlo multiple imputation algorithm to deal with the missing data. Clinical and psychosocial aspects and perceptions about diabetes care during the study were assessed using the Chi-square test. Data on patients’ perceptions of changes in habits that occurred during the pandemic were reported as the median ± interquartile range (IQR), and analyses were performed using the Mann–Whitney U test for the between-groups comparisons and the Wilcoxon Rank test for the within-group comparisons. Results of the questionnaires were analyzed for the presence of a positive screening result for the disorder based on previously cited cutoff values. Comparisons of positive screening between groups were performed using the Chi-square test/Fisher’s exact test and comparisons of within-group data were performed using the McNemar’s test. Comparisons within groups were performed post hoc and sought to assess changes from baseline to follow-up within each arm of the study. Two-tailed tests were used to determine significance at the 5% level.
Ethics approval and consent to participate
The informed consent form was read by the telephone contact for all participants who were included in the study. The terms were read and applied by the postgraduate students of the research group. Agreement was registered using an audio recording or an electronic message. All methods were performed in accordance with the relevant guidelines and regulations, and was approved by the institutional ethics committee (Comissão Nacional de Ética em Pesquisa—Nº 4059760). This trial was registered at ClinicalTrials.gov (registration: NCT04344210). This reporting follows the CONSORT statement18.
Consent for publication
All authors have reviewed the final version of the manuscript and agreed with the publication of the results presented.
